
Disclaimer: This series is for educational purposes and should not be considered medical advice. While we attempt to do our best to provide accurate and balanced information in this series, we always welcome input that will make it more useful for parents and the community. Also, please consult a physician and/or psychologist if you are looking for professional advice about these topics.
Our weekly series Parents Need to Know the Truth About Gender Choices and Gender Transitions concludes this week. Our goal has been provide detailed scientific and fact-based information in a format that we hope helps parents understand the topic better.
The segment concludes with the following three segments:
- Do transgender activists have a nefarious agenda?
- Is gender on a spectrum, meaning it has varying levels between two extremes? This one is a bit technical, but we feel it provides a good foundation for the terminology used in the discussions by the experts advising the schools.
What legal rights do parents and minors have in Maryland? Each state is different.
#3 Do transgender activists have a nefarious agenda?
At Transparency in Education, we haven’t found any evidence that this is the case, and are disheartened by those who have accused transgender activists of “grooming” children or trying to destroy nuclear families. Similar false accusations used to be made against homosexuals, also without evidence.
However, there are some online pro-transition transgender influencers whose influence can be fairly characterized as negative. In her book, Irreversible Damage: The Transgender Craze Seducing our Daughters, Abigail Shrier documented how some (but certainly not all) transgender influencers provide children and teens with inaccurate information and advice, including recommending medically transitioning even if they didn’t have gender dysphoria or identified as transgender.
These individuals, however, are not representative of the vast majority of transgender people. The vast majority of transgender people simply want the right to access psychological and medical care to help them gain a measure of peace in their lives by exercising their right to live in accordance with their gender identity. Our position is that we want to ensure that the right treatment is matched with the right patient to get the best results possible based on science. We support the right of consenting adults to make decisions about their own care and live in accordance with their gender identity, and don’t believe that supporting this will harm families or children.
We also vehemently support the right of parents to be informed about their own child’s mental health status by the public schools, including gender-related concerns. Currently FCPS’ policy 443 supports that children experiencing gender dysphoria receive affirmative-only therapy, a controversial approach lacking evidence of effectiveness. (See earlier segments in this series on treatments.) FCPS’ policy is to not notify parents that they are supporting this kind of therapy, unless they believe the child’s parents are supportive. Parents who would prefer a different approach will simply not be told, and the school will proceed with a therapeutic approach that the child’s parents object to. We think this is unconscionable, and schools should not be allowed to do this.
Gender dysphoria is not a “one size fits all” condition. There are different presentations of gender dysphoria and at least three kinds of therapy available to help children. We believe parents should get to choose the type of therapy used to support their children. We also believe that transphobia is a real phenomenon, and we support the rights of transgender people to be welcomed into society and have access to appropriate medical and psychological care, including the right to medically transition. FCPS supporting a controversial approach to therapy and doing it in secret without parental consent is the agenda we strongly oppose.
#2 Is gender on a spectrum, meaning it has varying levels between two extremes?
No, not if by gender one is referring to biological sex. Unfortunately, the distinction between biological sex and “gender”/”gender identity” are often confused in public debates, which is part of the challenge of discussing the issue.
The following is a bit technical but please bear with it as it is designed to provide the foundation for understanding the terminology and details of the situation in contemporary society.
Let’s start by explaining that gametes are mature reproductive cells found in humans. There are two types of human gametes: sperm, which are produced by males, and eggs, which are produced by females. A person’s biological sex is nearly always discernable by the gametes they produce or have the potential to produce. A person who produces sperm is male. A person who produces eggs is female.
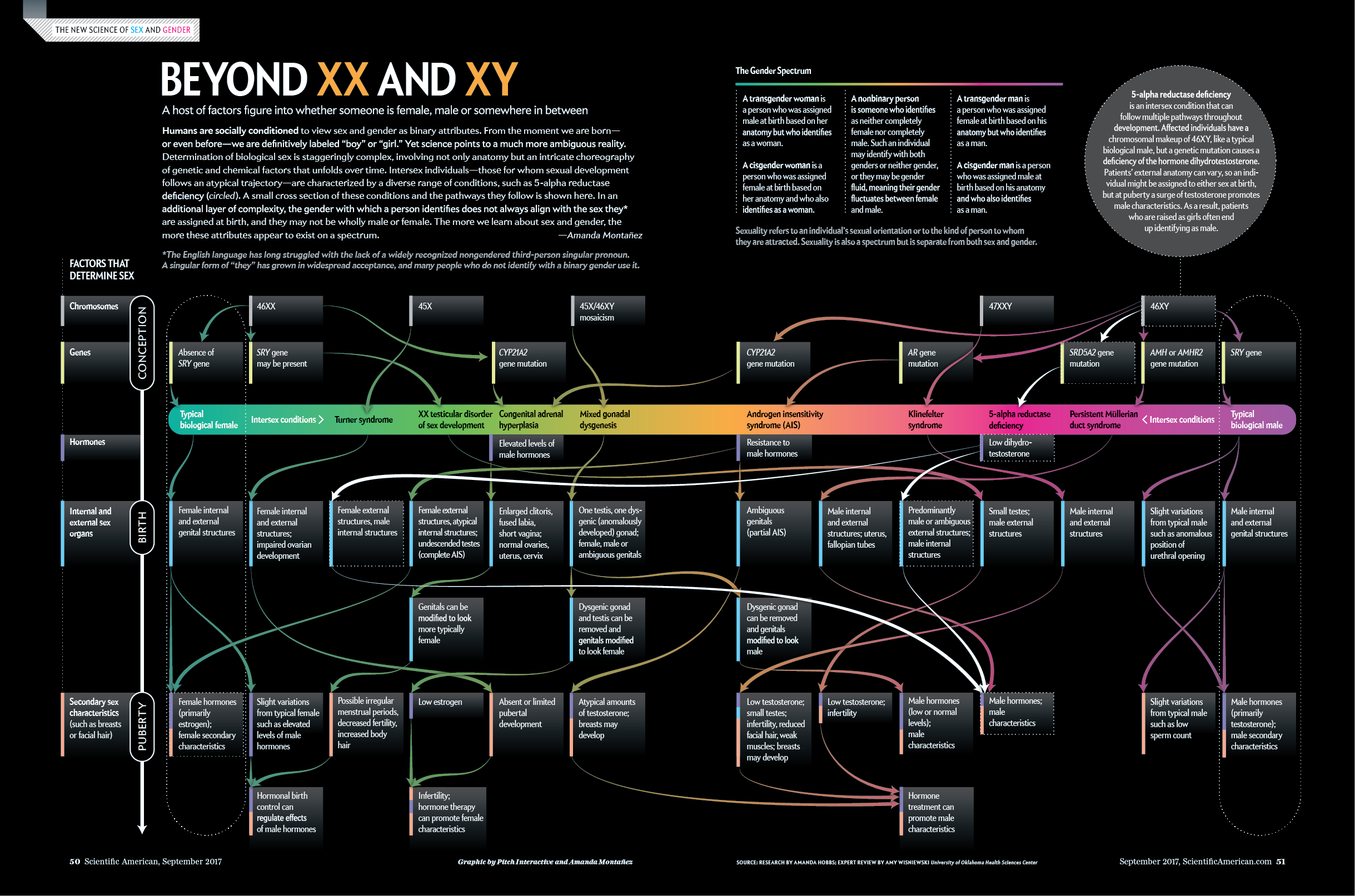
Prior to puberty, humans do not produce gametes, so biological sex is typically determined at birth by the presence of male or female anatomy due to the very high probability that most babies will eventually produce the gametes corresponding to their anatomy. There are exceptions to this general rule for intersex children, which are described below, but biological sex is determined by gametes, which are binary. There are no gametes “in-between” sperm and eggs. There are only two types.
Historically, science has accepted that there are only two biological sexes as determined by gametes. Some scientists have proposed presenting gender as a spectrum based on various intersex conditions. Critics regard this spectrum as simply defining a range of atypical sexual anatomy and don’t believe it establishes the existence of a third biological gender. Medical science has yet to find a case in human history of a person whose anatomy will allow them to simultaneously carry babies and impregnate biological females.
{kind=link}
With regard to people with an intersex condition, a person who has reproductive or sexual anatomy that would be considered atypical because it doesn’t fit the standard definition of male or female, such as someone who has both a vulva and testicular tissue, which is called ovotestis. Scientific research has found as many as thirty different types of intersex anatomy, including, for example, Klinefelter Syndrome, Androgen Insensitivity Syndrome, and Congenital Adrenal Hyperplasia. A person who is intersex will typically only produce a single type of gamete or be infertile. An intersex person may or may not identify as transgender and may or may not experience gender dysphoria.
However, gender identity is often thought of as a continuum, from the most masculine male to the most feminine male and the most feminine female to the most masculine female, with multiple stops in between. There is evidence suggesting (but not proving) that the brains of people with a transgender identity have shifted in the dimorphic parts of their brains towards structures that are more similar to cisgender people of the biological sex that corresponds to their gender identity, and these appear to be related to testosterone levels during pregnancy. (See Soh, Debra, The End of Gender, Prentice Hall, 2020, page 114-118.)
Newer terms such as “agender”, “genderqueer”, “non-binary”, “pangender”, “quadgender”, “gender-netural”, “genderfree”, “netrois”, “demigirl”, “demiboy”, “feminine-of-center”, “masculine-of-center”, “girlflux”, “boyflux”, “paragirl”, “paraboy”, “librefeminine”, “libremasculine”, “FTX”, “MTX”, and “genderfluid”, are just a few examples of ways in which some people describe their gender identity. Most parents are familiar with a more limited set of descriptions, such as “effeminate” (which some consider offensive), “transsexual” (usually considered a deprecated term) or “tomboy”. Parents may want to watch “Trans Kids: It’s Time To Talk” to learn more about the different experiences people have.
With these newer, more highly differentiated labels only recently being added to the vocabulary of gender identity, scientists have not yet conducted studies to determine if these identities correspond to finer-grained differences in the brain, genetics, or other biological structures or processes. Even if such evidence is not discovered, this doesn’t mean that using either the older or newer terminology to describe one’s own internal personal experience is invalid.
So why is this issue of what a man is and a woman is so contentious? Isn’t that determination obvious in the vast majority of cases? As Genspect.org explains, some people have a belief systems based on gender theory that posits that we all have an invisible gender identity within us and that some of us have been born in a body that is not matched with our gender identity. Others do not subscribe to this belief and consider themselves “gender critical.” Gender critical theory argues instead that we are simply born in — and as — bodies, and although gender roles are imposed upon us, these need not be perceived as an identity. They can simply be rejected: many just learn to live with certain gender roles. The biopsychosocial model suggests that a combination of biology, psychology, and society will drive certain behaviors, which manifests as our identity. The differences between these viewpoints seem to be the root of the majority of the controversy that currently surrounds gender politics.”
It’s important to point out that not everyone has an internal sense that they have a gender identity. The term “gender identity” arose out of research with intersex individuals and is a useful way to think about the incongruence between their biological sex and their internal experience of gender, but it isn’t necessarily applicable to most people.
Statements such as “transwomen are women,” however, aren’t scientifically accurate. Hardly anyone would dispute the fact, for example, that some biological males have a genuine and deeply felt internal sense of being female. Their biological sex, however, is male. While some biological males who are transgender insist that they be accepted as “real women” and regard anyone who disagrees as insulting or transphobic, others disagree.
At Transparency in Education, we believe it is important to draw a distinction between biological sex and gender identity. We want to keep the terminology clear to ensure that discussions about drugs and other treatments, which can affect biological males and biological females differently, aren’t made more confusing by using the language of identity rather than the language of biological science. Drawing that distinction is in no way meant to deny the very real internal sense of identity that transgender people have. We are just trying to use easier-to-understand vocabulary about a topic that can be very complex.
#1 What legal rights do parents and minors have in Maryland?
Disclaimer: The following answer is not intended to be legal advice and is based on the current regulations.
At present, Maryland law does not allow minor children to consent to medical and mental health treatments without parental consent before the age of 12 and limits the conditions under which a child can consent, such as life-saving measures and pregnancy. While a child may self-refer and consent to mental health treatment at age 12 without parental consent, minors do not have a right to refuse a mental health treatment that a parent chooses. Maryland is not currently offering puberty blockers or cross-sex hormones at our public schools, and our law does not specifically allow it, but it doesn’t prohibit it either. Parents do have the right to access a minor child’s medical records, since HIPPA privacy laws do not apply to schools.
The state of California has made both puberty blockers and cross-sex hormones a right for minors under its law and has passed legislation making it a “sanctuary state” for out-of-state children to travel to and receive puberty blockers, cross-sex hormones, and affirmative therapy in secret. The California Teachers Association has pursued legislation that would allow students to leave school during the day to obtain puberty blockers and cross- sex hormones without parental consent.
Transgender rights advocates have sought to make gender transition a human right. If this becomes accepted as a right for minors in Maryland, the legal implication is that parents could lose the ability to control their child’s medical treatment. It has become considerably more extreme elsewhere. In Canada, a father was jailed for speaking against his daughter’s gender transition, and in California, a father lost custody of his child who he didn’t believe was transgender. We know of no push for such measures in Maryland and do not see them promoted in any discussion. We mention these examples because we wonder if, a few years ago, the parents mentioned above thought this could never happen where they lived. The laws of progressive states and nations are no longer predictable using historical logic.
Additionally, there is the issue of whether gender identity is an immutable (or unable to be changed) part of a person’s identity. To fall within the protection of the Equal Protection Clause, a protected personal attribute (such as biological sex) must be “immutable”. Changeable attributes such as hair color are not protected. Transgender rights advocates often claim gender identity is immutable, which would have the desired legal effect of falling within the Equal Protection Clause.
The fact that gender identity is known to be flexible in children, the existence of detransitioners (who returned to their original biological sex after transitioning to the opposite gender) and desisters (who experienced gender dysphoria that resolved), and the existence of adults who experience gender fluidity, calls into question whether gender identity is immutable over the course of a lifetime. Whether or not it is immutable, gender identity is considered protected under Title VII of the Civil Rights Act of 1964, though this has been subject to multiple ongoing court challenges.
So what can parents in Frederick County do about all of this? We can support parental rights policies and legislation as has been done in other states, and return control of the education process to parents and build a collaborative relationship between the school system and the community through parental empowerment.
Part 6 of our series on Gender Dysphoria and Transgender Choices
This week continues our series on providing a fact-based program for parents on the definition and impacts of gender dysphoria (or confusion) and transgender decisions. The series also provides relevant references to FCPS’s approach.
Since public schools, including FCPS, have installed policies that restrict and sometimes prohibit parents from knowing what choices their child makes regarding gender, we feel this is critical information for families.
In this second to last installment, we cover whether medical transitions work and help parents understand the relevancy of Rapid Onset Gender Dysphoria.
#5 Do medical transitions help?
For some people, yes, but they come with serious complications and risks. Medically transitioning via cross-sex hormones results in irreversible secondary sex characteristics. Surgical procedures, including facial reconstruction, double mastectomy, breast construction, gonadectomy, and phalloplasty, involve risks in terms of undesirable health outcomes (infertility, infection, sepsis) and may result in less-than-desired cosmetic outcomes. Maintaining the appearance of a different biological sex than a person’s biological sex requires lifelong hormonal treatment, which carry risks including hypertension, vaginal atrophy, higher cancer risk, stroke, liver damage, and bone mineral loss.
Some people who medically transition have regret and detransition, while others are satisfied with the result. Approximately 25-35% of transgender people pursue medical transitioning of some sort. There is currently no validated method to determine the likelihood of whether a person will or won’t desist prior to medically transitioning. There are serious risks associated with medically transitioning, though most experts agree that in some cases medically transitioning is the most appropriate treatment.
There is very little evidence of the number of people who transitioned away from their biological sex and then de-transitioned back to their biological sex. These people are called “de-transitioners” and include Keira Bell, who famously won her lawsuit against the Tavistock gender clinic in the UK, which found that children under age 16 cannot reasonably consent to sex reassignment operations. You may be interested in learning about her story here.
There is currently limited data available on the reasons people choose to de-transition. One study found that common reasons include trauma (including sexual trauma) that contributed to their transgender identification; homophobia and difficult accepting oneself as homosexual; peers, social media and online communities that influenced their development of a transgender identification and desire to transition; health concerns; dysphoria rooted in misogyny; and finding alternatives to deal with their dysphoria. External factors such as a lack of support, financial concerns, and discrimination also occurred and were less common.
The rates of de-transition from both social and medical transitioning have not been reliably established at this time due to a lack of research, and are currently a subject of debate. One challenge with collecting this data is that less than 0.25% of people who detransition report their detransition to the doctor who facilitated their transition and change to a different doctor. (See here at 49:07)
Here at Transparency in Education, we support the right of people to medically transition, but hope this is a measure of last resort after other less invasive approaches has been explored, including therapy, which can help resolve underlying issues that many de-transitioners realized too late were the real sources of their desire to undergo permanent physical changes. In our view, this looks a lot like a medical malpractice, similar to the opioid crisis in which faulty scientific evidence led to overprescribing these addictive drugs.
The same lack of scientific evidence is happening again for the standards of care for children with gender dysphoria. We explained that in a previous question in this series: Do experts agree on the standards of care for gender dysphoric children?
#4 What is Rapid Onset Gender Dysphoria, “glitter families,” and why are these terms important for parents to know?
Kids today spend a lot of time online, and there are documented cases where adolescents were influenced by transgender influencers’ videos in which they instill fear and anxiety in adolescents by suggesting that they need to transition as soon as possible so they won’t end up killing themselves. (See Shrier, Abigail, Irreversible Damage, Regnery, 2020, page 50, 55, 220) The advice these influencers gave included statements such as, “if you’re asking the question ‘Am I trans,’ the answer is probably yes” and “[Y]ou don’t need to be a hundred percent sure you’re trans to try hormones,” both of which are inaccurate and unethical. (Irreversible Damage, page 48)
Some influencers have coached children to answer clinicians’ questions with made-up stories about their gender dysphoria so they’ll get a diagnosis that will allow them to obtain puberty blockers or cross-sex hormones. (Irreversible Damage, page 52). Some online influencers encourage children whose parents don’t support their transition to establish a “glitter family” of online contacts who “truly understand them” who will support the child’s choices. (Irreversible Damage, page 51). This can create a situation in which children are alienated from their families at a time when they need their support most. Aaron Kimberly, who transitioned from female to male and has an intersex condition, has also been outspoken in his opposition to current trends in transgender care and education, stating that students are “picking up a culture, not evidence-based clinical information.”
It’s important to say that none of this means that transgender identities, in general, should be regarded as invalid or suspect, only that parents and school staff need to be aware that in some cases, children’s interest in transitioning could be influenced by fear and/or inaccurate information from social media or other sources. Unfortunately, FPCS has mandated an affirmative-only approach to dealing with gender dysphoria, which means they won’t explore other causes and will simply confirm to the student that their interest in transitioning will be honored at school, which overlooks the real possibility that this interest in transitioning is based on fear or misinformation, not a genuine transgender identity.
In her community, Dr. Lisa Litman started noticing that a few children started announcing that they were transgender. Originally, she thought this was great that people were more open about this issue, but after the first few announcements even more announcements occurred, which got her concerned. She realized that the number of adolescent girls declaring that they were transgender was well above the expected rate of occurrence for such a rare condition, especially since this condition was historically found nearly exclusively in young boys, not teenage girls. She began to conduct research in this area, eventually coining the term Rapid Onset Gender Dysphoria (ROGD) to describe this phenomenon, which is documented in this paper.
This term describes the relatively recent phenomenon, typically involving female adolescents who suddenly develop an interest in transitioning despite no gender dysphoria in early childhood and a history of gender expression that aligned with their biological sex. Parents have described that the onset of gender dysphoria seems to occur in the context of belonging to a peer group where one, multiple, or even all a child’s friends have become gender dysphoric and transgender-identified during the same timeframe and that their children exhibited an increase in social media/internet use prior to disclosure of a transgender identity. This is not currently a clinically accepted term or diagnosis. Dr. Lisa Littman proposed this as a subtype of gender dysphoria in a paper in 2018, and it is an area of active research.
In other words, ROGD is a social contagion. To quote Dr. Littman from her interview, “It’s plausible that a set of beliefs can be shared from person to person, and in groups, that… symptoms should be interpreted as gender dysphoria, proof of being transgender, (that) the only way to feel better is to transition, and the belief that anyone who disagrees with you is abusive, transphobic, or something like that. And it’s those sets of beliefs, in my opinion, that can definitely be shared person to person, and could lead a vulnerable kid to come to the conclusion that they are transgender and they need to transition.” With regard to de-transitioners, she said, “The science is not settled. In terms of talking about people in this study, more than half felt that the evaluation they got was not adequate before they transitioned…. There seems to be a lot of effort in not hearing the stories that would challenge the narrative that some people are hurt.”
At Transparency in Education, we think this is very sad and concerning, and we strongly encourage parents to watch Dr. Littman’s interview about this topic.
Some of the girls who experience Rapid Onset Gender Dysphoria went on to use puberty blockers and cross-sex hormones. Puberty blockers are supposed to be a safe “pause button” that buys time for children to consider their gender identity before developing secondary sex characteristics. But is that true? We answered that in a previous question: Are puberty blockers safe and reversible?
Part 5 of our series on gender dysphoria and gender transition includes two questions:
- Do experts agree on the standards of care for gender dysphoric children?
- Does teaching Gender Identity to Children Create Concerns in Children they might not have had otherwise?
#7 Do experts agree on the standards of care for gender dysphoric children?
The World Professional Association for Transgender Health (WPATH) was started in 1979 and has produced a Standards of Care document to provide guidance to medical practitioners for providing care to gender dysphoric and transgender patients. They are currently on their eighth edition of the standards, which has been highly controversial and even called bizarre by reputable psychologists, who believe the standards have such glaring issues that this once renowned organization has become discredited.
In 2006, the 6th edition of WPATH Standards of Care set standards for medically transitioning, including requiring patients to live in their gender identity for a year and getting a referral from a psychologist before obtaining surgical interventions. In 2012, the 7th edition of the WPATH Standards of Care removed the one-year requirement and recommended psychotherapy prior to transition but no longer required it. The 8th edition of the WPATH Standards of Care removed any requirements to obtain a diagnosis of gender dysphoria and no longer includes minimum age requirements for medical treatment, and removed a chapter on ethics. These changes in the Standards of Care have been criticized by medical professionals for not providing sufficient safeguards to ensure patients will be properly assessed to ensure they receive the appropriate treatments. Others have claimed that WPATH is an organization “captured by activists”. Those in favor of the standards argue that these changes eliminate “medical gatekeeping” that could prevent transgender people from getting the care they need.
We encourage parents to view the new, controversial standards and judge for themselves, as well as this expert critique, which explains, “There is a disregard for parental authority by advising clinicians to prescribe hormone treatment to children without parental support. This creates triangulation, where the parent is deemed the persecutor, the child is the victim, and the clinician is the apparent savior. It is an unhealthy situation and causes unnecessary distress within families at an already very stressful time. WPATH’s advice will lead to alienation of parents as they advise clinicians to “challenge” parents who are considered unsupportive because of any concerns about early and aggressive medical procedures.”
We are concerned that since FCPS has decided to allow children to secretly transition their gender without parental approval, they will use these standards against parents, claiming that they are simply following the WPATH guidance without acknowledging that it is highly controversial and lacks evidence. Even more concerning is that other American medical and psychological associations have adopted similar affirmative-only approaches, also ignoring the evidence.
So what’s a parent to do? Parents who want a different approach might want to order this book on gender dysphoria therapy that is ethical and based on evidence but also have other options. With the opioid crisis, patients began suing their doctors, which resulted in greater controls over prescribing addictive drugs. There are currently lawsuits in other countriesattempting to do that for gender dysphoria treatments, including ones filed in Montgomery County, MD.
Currently, FCPS plans to teach even more about gender identity topics. Does this cause harm, and should Frederick’s parents sue FCPS? We’ll address the legal rights of parents in our last set of questions in two weeks.
#6: Is teaching about gender identity and/or providing an environment that treats gender as a choice creating concerns in children they might not have had otherwise?
“Iatrogenic” is a medical term that refers to a medical or psychological treatment that causes an illness or health condition, such as getting an infection after knee surgery. Some researchers think teaching about gender identity could be iatrogenic and might cause students to have gender identity concerns they might not have had otherwise. Up until recently, gender identity as an option was not a topic commonly taught or accepted in public schools, especially in elementary schools, so we don’t have enough data to draw from. It is fair, however, to say that because not enough data exists that by teaching these topics, the public schools are conducting an experiment.
That’s why we believe parents have a fundamental right to opt-in to the schools teaching this material. The power of suggestion is a real phenomenon, and many parents don’t want to risk confusing their child. The reason we have rejected the opt-out approach is that its misleading parents to believe they can control what their child is being told at school on this topic. It is possible a parent may not realize that these topics are being presented based on the wording used in school communications sent early in the year, or they missed the email announcing the opt-out option, or their child lost the opt-out form on the way home from school. But more important for parents to know is that, as we have shown, gender choice and expression are embedded within other activities and subjects. Math questions are now pronoun neutral and exclude references to girls and boys. FCPS counselors use materials that normalize gender choices for children. Dr. Cuppett, Executive Director of Curriculum and Innovation at FCPS, has acknowledged that this topic is being introduced in non-instructional activities, and there have been published examples of teachers actively soliciting pronoun choices under the umbrella of getting to know their students. It is important that parents be aware that their children are in an environment at school where the ability to choose a gender is considered acceptable and normal, and opting out of a health class (or even opting in) is not effective if you wish to deal with these topics solely within your family.
As Abigail Shrier explains in her book, schools are starting to teach kindergarteners that “biological sex and gender very often come apart; one has no essential connection to the other.” Of course, that’s false, since historically for 99.99% of people their biological sex and internal sense of their own gender match. Additionally, she explains, schools are increasingly teaching stereotypes, such as the idea that “Girls who like math, or sports, or are logical; boys who sing, or act, or like to draw are all ‘gender nonconforming.’” Gone are the days when we told kids they could just be kids and pursue whatever they are interested in. Now we label them as gender-conforming or nonconforming.
Additionally, Shrier points out the curricula that are used to teach these concepts are often developed by national advocacy groups, not local educators, and introduce children to The Genderbread Person and the Gender Unicorn. We encourage parents to take a look at those resources and decide if this makes sense to teach to elementary students. Shrier also documented that middle schools often use Positive Prevention PLUS, which asks students to “imagine they are a different gender” and even “What would be fun about being another gender?” (Note; we have found no evidence of this last activity in FCPS.
It’s not too hard to see the path this sort of instruction could contribute toward creating. If the concerns of parents and some researchers are right, this instruction is priming the pump for children to question their gender identity who otherwise wouldn’t have and is suggesting that not identifying with one’s biological sex is common. Because schools often praise students who “come out as transgender” (or what might be more accurately seen as expressing their gender dysphoria since it takes time to develop a stable transgender identity), their social status rises. And given a choice between all sorts of interesting labels like genderqueer and nutrois, surely some kids will avoid the more vanilla labels like cisgender just to be different.
Couple that with the normal awkwardness about puberty and possible unresolved questions about their sexuality or underlying trauma or psychological conditions, and some kids will decide that what they really need to feel better is to socially transition, which they can do in secret at school without getting a clinical diagnosis since medical organizations no longer require that and schools now refrain from telling parents. When socially transitioning doesn’t resolve their gender dysphoria, they might start requesting puberty blockers. As discussed in previous parts of this series, children who take puberty blockers, which are associated with persisting gender dysphoria, go on to take cross-sex hormones in nearly 100% of cases. Cross-sex hormones will cause permanent physical changes, and some students will even opt for surgical procedures after that once they reach the age of consent.
Science hasn’t determined how many children will go down this path, but we know this path does occur for some children. There are multiple organizations focused on the needs of de-transitioners who regret going down this path. We at Transparency in Education support the right of consenting adults to socially and medically transition, but don’t think it makes sense for schools to push gender ideology on kids, and that parents’ rights to not have their children taught this material should be respected.
Part 4:
#9: Are puberty blockers safe and reversible?
Taking puberty blockers comes with significant risks. In July of 2022, the FDA added a warning that the drugs commonly given as puberty blockers (gonadotropin-releasing hormone agonists) are a serious risk for youth who take them.
Using puberty blockers to delay puberty for gender dysphoric children is an off-label use and not approved by the Food and Drug Administration. The long-term physical and psychological effects of taking puberty blockers and delaying puberty are not fully understood.
Puberty blockers have historically only been given to children that experience an early onset of puberty, but the current standard of care is that they should not continue taking puberty blockers past age 7, due to the health risks, including bone mineral loss that can lead to fractures.
Here are some facts regarding puberty blockers:
- Some scientists have found evidence that puberty blockers cause depression and other emotional disturbances related to suicide.Discussing an experimental trial of puberty blockers in the U.K., Oxford University Professor Michael Biggs wrote, “There was no statistically significant difference in psychosocial functioning between the group given blockers and the group given only psychological support. In addition, there is (unpublished) evidence that after a year on [puberty blockers] children reported greater self-harm, and that girls experienced more behavioral and emotional problems and expressed greater dissatisfaction with their body—so puberty blockers exacerbated gender dysphoria.”
- Taking puberty blockers will prevent children from developing sexually and may make experiencing a normal sex life difficult, depending on how developed a child’s sexual organs are prior to taking them. Puberty blockers are most commonly prescribed in a stage of sexual development (medically known as Tanner Two stage) that will result in them being unlikely to achieve orgasm if they continue with the blockers and then proceed to cross-sex hormones.
- Puberty blockers may delay the development of a child’s brain. In July of 2022, The New York Times published an article The Battle over Gender Therapy
by Emily Bazelon. In the article Bazelon reported, “Little is known about the impact (of puberty blockers) on brain development.” In June the June 2022 The Royal Children’s Hospital of Melbourne published a newsletter indicating that after several years of assuring families that puberty blockers are reversible a study will be undertaken to determine their effect on the “still maturing adolescent brain.” The point is that although the impact on the brain is unknown, the suppression of natural hormone release, which is the function of puberty blockers, is believed to be a significant risk to brain development. - Nearly 100% of people who start taking puberty blockers later start taking cross-sex hormones. In other words, while taking puberty blockers is usually presented as a “pause button” so children can consider their options, in nearly all cases, it is simply a step along the way to a full medical transition with cross-sex hormones. If a person has not undergone puberty before taking cross-sex hormones, they are at risk to becoming permanently infertile. For biological males, taking puberty blockers can make it impossible for them to medically transition to female via vaginoplasty, since there may not be enough tissue available to perform the operation.
The bottom line is that the risks associated with puberty blockers are often downplayed in the public conversation about them. It’s important for parents to understand that taking them isn’t a neutral “pause button” but can have significant psychological and physical effects that need to be considered.
The same can be said about medically transitioning via cross-sex hormones and/or surgical procedures such as a double mastectomy or castration, often euphemistically called “top surgery” or “bottom surgery”. Next week we’ll present the evidence about medical transitions, answering the question: Do medical transitions help?
#8: Does socially transitioning resolve gender dysphoria?
No. In fact, socially transitioning is associated with persisting gender dysphoria, as found here and here. Though some evidence suggests that children who socially transition experience short-term relief from gender dysphoria and a reduction in suicidal ideation, gender dysphoria experts Dr. Michael Bailey and Dr. Ray Blanchard have stated, “[T]he best scientific evidence suggests that gender transition is not necessary to prevent suicide…There is no persuasive evidence that gender transition reduces gender dysphoric children’s likelihood of killing themselves.”
Socially transitioning is reversible in the sense that it involves temporary cosmetic and name changes, but the long-term psychological effects of socially transitioning and then desisting are not known. For biological females, socially transitioning can involve binding their breasts, which poses health risks such as back, shoulder, and chest pain, shortness of breath, bruised and fractured ribs, and lung function. Tucking (for males) lacks long-term studies, but several studies suggest that this can impact fertility by causing cryptozoospermia and testicular torsion.
Socially transitioning back to a gender identity that matches one’s biological sex often causes children stress and anxiety, and some children who no longer experience gender dysphoria will be reluctant to transition back.(See Soh, Debra, The End of Gender, Prentice Hall, 2020, page 91, 178-188.) Some scholars have arguedthat socially transitioning is iatrogenic (induced unintentionally either medically or psychologically through facilitation, support, and encouragement by others) and leads to medical transitioning, though this has not been established (see here and here). Schools affirming a student’s gender identity or publicly celebrating a transgender student’s courage are not neutral actions, and can unintentionally influence students’ identity formation.
Parents should be aware of their children’s choices and actions and be given the opportunity to provide or deny consent to schools to allow them to support the social transition of their child (that is, the parents must aware, involved, and in control of the decisions and the activities). The best guidelines for schools doing this that we’ve found were published by Genspec.org, an international organization supporting evidence-based approaches to gender issues. We provide a few examples of their advice for supporting students who are socially transitioning below, and encourage parents to visit their entire web site to learn more. FCPS has not adopted any of these model guidelines.
- Names and Pronouns – “Teachers and other school staff should acknowledge the responsibility of their position and be careful not to give an official (sanction or approval) on any given name: this may inadvertently (shut down) further exploration of a vulnerable student’s identity exploration. Some gender non-conforming young people go through a series of different names, so it might not be helpful to concretize a current chosen name. If parents have concerns about the name that a child is going by in school, these should take precedence over the child’s desires, and parents should not be cut out.”
- Deadnaming/Misgendering – “Misgendering” is a term to describe the situation when, for example, a teacher refers to or addresses a person with language that inaccurately represents the person’s inner sense of gender identity. Although this can be perceived as harmful to an individual, there is no quality evidence that supports this perception; nor is there evidence available to demonstrate the impact of referring to a person with terms that do not align with their biological sex. We recommend that school authorities use biologically accurate language in all cases. We caution against equating “misgendering” with violence, or making other hyperbolic comparisons. Unless a wider pattern of bullying or other malicious behavior is taking place, “misgendering” should not be punishable.
We are concerned that FCPS current policy goes against these recommendations, which were developed by psychologists with extensive experience working with children and schools with gender-questioning children. We know that this is already affecting other students. As we’ve reported more than once, an FCPS parent testified during a recent Board of Education meeting that his daughter had to meet with a counselor for several hours after referring to another child by their given name. That parent’s public comments are available on a link to the video of his public comments in one of our previous articles.
But…maybe all of this makes sense. After all, isn’t gender on a spectrum? Shouldn’t we just accept this “new normal” of gender identity as a more accurate way to think about how people identify? Our answer to that will come next week we tackle the following question: Is gender on a spectrum, meaning it has varying levels between two extremes?
Part 3:
#11: Are gender dysphoric and transgender people at a greater risk of suicide?
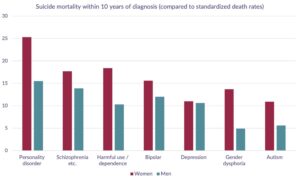
Yes, but there is controversy in this area. There is no high quality evidence that the most commonly cited suicide rate of 41% is correct, and the study from which this statistic came has been criticized for its methodology. A Swedish study found that suicide rates for personality disorder, schizophrenia, substance addiction, bipolar and (among males) depression and autism were all higher than suicide rates for gender dysphoric people, and that “it is difficult to distinguish one [gender dysphoria] from the other [mental health conditions] with regard to suicide risk.” This same study found that the suicide rate was 0.6% for gender dysphoric people.
People with gender dysphoria do have a suicide rate that is higher than the general population, but that rate is still lower than those with other conditions, as the following graph shows.
Unfortunately, some therapists encourage parents to support socially and/or medically transition their child, saying that their choice is between “having a dead daughter or a live son” (for transgender males) or “having a dead son or a live daughter” (for transgender females). Some have questioned this heavy-handed approach as being unethical, since given that choice even the most reluctant parents are likely to agree to a transition.
There is little evidence that medical transition decreases suicidality. One study showed that adults who underwent sex reassignment surgery were actually 4.9 more likely to have made a suicide attempt and 19.1 times more likely to have died from a suicide attempt. Another study concluded that after undergoing sex reassignment that transgender people have “considerably higher risks” for suicidal behavior. The European Journal of Endocrinology found that male-to-female transgender people had suicide rates 51% higher than the general population after treatment with cross-sex hormones.
So what’s going on here? Why are so many children and adolescents encouraged to transition to a different gender when doing so doesn’t appear to decrease suicide risk, and might actually make it worse? We’ll explain that next time, but we’ll give you a hint now. Part of the answer is found in the question: Is there only one kind of gender dysphoria?
#10: Is there only one kind of gender dysphoria?
There are three officially recognized pathways to developing gender dysphoria recognized in the Diagnostic and Statistical Manual (DSM-5), including child onset gender dysphoria, late onset gender dysphoria, and gender dysphoria associated with disorders of sexual development. There is a fourth proposed type called rapid onset gender dysphoria. Additionally, sometimes other trauma or psychological conditions can present as gender dysphoria, but are actually manifestations of these other conditions. Let’s go through each type and explain it.
Child Onset Gender Dysphoria – This is the most common case, with 75% of transgender males and 72% of transgender females first experiencing gender dysphoria by the age of 7 and over 80% of both males and females reporting that experiencing gender dysphoria was one of their earliest childhood memories. Around ~80% of children with this presentation desist at or through puberty without intervention. This presentation is highly correlated with later homosexuality
Late Onset Gender Dysphoria – This presents in adolescents and adults and is related to transvestic disorders with autogynephilia. This is seen almost exclusively in non-homosexual boys and men who are gender conforming as children. (Autogynephilia is a condition in which men are sexually aroused at the thought of themselves being a woman).
Gender Dysphoria Associated with Disorders of Sexual Development – This presents in people who have rare intersex conditions, such as one’s chromosomal sex not matching one’s biological sex characteristics. Not all people with disorders of sexual development have gender dysphoria, but a small percentage do. Females with a disorder of sexual development called congenital adrenal hyperplasia, for example, are more likely to be same sex attracted, choose male typical occupations, and are more likely to experience gender dysphoria.
Rapid Onset Gender Dysphoria – This term describes the relatively recent phenomenon, typically involving female adolescents, who suddenly develop an interest in transitioning despite no gender dysphoria in early childhood and a history of gender expression that aligned with their biological sex. Parents have described that the onset of gender dysphoria seems to occur in the context of belonging to a peer group where one, multiple, or even all a child’s friends have become gender dysphoric and transgender-identified during the same timeframe, and that their children exhibited an increase in social media/internet use prior to disclosure of a transgender identity. This is not currently a clinically accepted term or diagnosis. Dr. Lisa Littman proposed this as a subtype of gender dysphoria in a paper in 2018 and it is an area of active research.
Comorbid Psychological Conditions – Medicine uses the word “comorbid” to describe conditions that can occur together, such as a person who has both depression and diabetes, where either condition can impact the other condition. For example, people with depression often don’t engage in enough self-care to manage their diabetes. The same can happen for gender dysphoria, which can be a manifestation of underlying trauma or psychological conditions.
Dr. Kenneth Zucker, an internationally recognized expert who oversaw the writing of the definition of gender dysphoria for the DSM-5 and helped write the 7th edition of the World Professional Association for Transgender Health’s (WPATH) Standards of Care has stated that just because a person is fixated on gender as a source of their problems doesn’t mean that transitioning will alleviate their distress. “There are different pathways that can lead to gender dysphoria, but it is an intellectual and clinical mistake to think there is one single ‘cause’ that explains gender dysphoria,” he said. (See page 124 of Irrerversible Damage: The Transgender Craze Seducing our Daughters) Dr. Zucker, who has sometimes advised his patients to medically transition, recommends that clinicians examine the entire person rather than immediately accepting someone’s self-diagnosis of being transgender.
People with gender dysphoria are over four times more likely than the general population to suffer from mental health problems and 58% of those with rapid onset gender dysphoria had a poor or extremely poor ability to handle negative emotions productively. This study and this study have found a connection between autism spectrum disorders (which involve intense interests and repetitive behaviors) and gender dysphoria. Another study found a link between Obsessive Compulsive Disorder (OCD) and gender dysphoria, in which symptoms can include an obsession about one’s gender. Another study found that about 15% of transgender youth had attention deficit hyperactivity disorder (ADHD) and that youth with ADHD were 6.6 times more likely to express gender variance than participants without ADHD.
Our point isn’t to try to deny the existence of genuine transgender identities, which are real, or to suggest that being transgender is always the manifestation of an underlying trauma or psychological condition. But we are saying these causes happen frequently enough that medical ethics require them to be considered them when evaluating people who present with gender dysphoria. It is also important to consider that in ~80% of children child onset gender dysphoria resolves without any intervention. Unfortunately, the affirmative-only approach that FCPS had written into its policy and regulation does not consider the full range of gender dysphoria presentations and treatments, and prematurely closes off therapists’ ability to consider the entire child and provide an individualized treatment approach.
But…since FCPS has taken the position that parents can be restricted from knowing what gender and transition choices their children are making there must be lots of evidence supporting the affirmative-only approach, right? After all, isn’t socially transitioning by changing a child’s names, pronouns, and other non-permanent attributes known to be harmless? Stay tuned for next time when we examine question #8: Does socially transitioning resolve gender dysphoria?
As always, if there are any questions or comments, please send them via [email protected].
Part 2: The second installment of our 8-part, 15-question series is designed to help parents get a clear picture of gender dysphoria and transgender transitions by presenting the known data and history from a scientific and medical perspective.
This week we provide answers to two questions.
- Why is gender dysphoria becoming more common?
- What therapies are available to treat gender dysphoria, which ones are the most effective, and which one does FCPS support?
As always, if there are any questions or comments, please send them via [email protected].
Question #13: Why is gender dysphoria becoming more common?
Science cannot yet explain the enormous recent rise in transgender identification, which is unprecedented. From 2017-2022, the number of youth who identify as transgender in the United States has doubled, with people between the ages of 13-17 identifying at a rate of 1.4%, all adults identifying at a rate of 0.5%, and adults aged 65 or older identifying at a rate of 0.3%.
Historically, gender dysphoria was found in 0.01% of the United States population (mostly boys). Prior to 2012, there was little to no scientific literature about girls aged 11 to 21 having ever developed gender dysphoria. (See Irreversible Damage, page xxvii, and this research paper.) Currently, most gender dysphoric children are female at a ratio of approximately 2:1, which is obviously a dramatic shift from gender dysphoria being a nearly all-male, rare phenomenon.
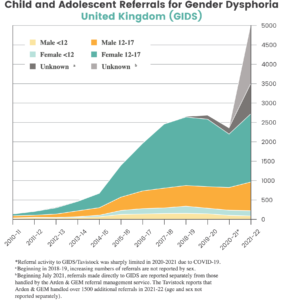
This dramatic rise has been observed in other western countries, such as the United Kingdom, which has experienced a 4,500% increase in referrals for gender dysphoria, as illustrated by the following graph.
As mentioned, there is currently no accepted scientific explanation for the recent rapid rise in gender dysphoria overall or for why females are now experiencing it at a higher rate than males. Some have proposed that greater social acceptance has enabled more people to self-identify and regard this as a healthy development, while others have proposed that impressionable children are being influenced by their peers, the internet, and pro-transition activists to inaccurately conclude they are transgender instead of in other clinical categories. The relative contributions of each of these proposed causes or the existence of other possible causes (such as better data collection or environmental changes) are not well understood or agreed upon.
Data suggests that the internet has played a role in a non-clinical phenomenon called Rapid Onset Gender Dysphoria, in which adolescent females suddenly develop an interest in transitioning despite having no gender dysphoria in early childhood and a history of gender expression that aligns with their biological sex. Parents have described that the onset of gender dysphoria seems to occur in the context of belonging to a peer group where one, multiple, or even all a child’s friends have become gender dysphoric and transgender-identified during the same timeframe and that their children exhibited an increase in social media/internet use prior to the disclosure of a transgender identity. This is not currently a clinically accepted term or diagnosis. Dr. Lisa Littman proposed this as a subtype of gender dysphoria in a paper in 2018, and it is an area of active research.
There are other possible (but not proven) factors at play. This rapid rise in gender dysphoria has occurred at a time when schools are increasingly teaching young children about gender identity, which some have argued may plant a seed in children’s minds that the vast majority of students wouldn’t have had if it had not been for the schools. Most people don’t have an internal sense that they have a gender identity separate from their biological sex. It’s possible that teaching about the concept of gender identity, which is done with the well-meaning intention of being inclusive and preventing bullying, does more harm than good for most students and actually causes confusion. Question # 2 will address this aspect of gender dysphoria/confusion in week 7 of the series.
We think a less controversial approach is needed. Instead of having schools introduce the topic of various gender expressions, we believe schools can emphasize that everyone is entitled to be treated with respect and that bullying for any reason is not acceptable. We believe the role of the school is to foster a tolerant and caring approach to all students. It is not the role of the school to influence identity formation.
But…some might ask, don’t kids with gender dysphoria and transgender identities have a higher risk of suicide than other populations? Don’t the schools need to do something to support these kids? We’ll tackle that one next time with question #10, Are gender dysphoric and transgender people at a greater risk of suicide?
Question #12: What therapies are available to treat gender dysphoria? Which ones are the most effective?
According to Dr. Debra Soh’s book on the topic, there are three main approaches to treating gender dysphoria: Affirmative Approach, Wait and See Approach, and Developmental Approach.
The Affirmative Approach is the most aggressive option and involves the child changing his or her name and pronouns and living as their gender identity at school. This psychosocial intervention exerts a powerful influence on a child’s development. There are no long-term studies that support the effectiveness of this approach. Studies have found that an affirmative-only approach prolongs a child’s gender dysphoria.
The DSM-5 is the main reference for psychologists that lists all the known mental conditions. Dr. Kenneth Zucker, an internationally recognized expert who oversaw the writing of the DSM-5 section on gender dysphoria, has argued that the Affirmative Approach is likely to lead children to pursue medical transitions. In other words, it is what clinicians call “iatrogenic”—a treatment that creates a new problem.
The Watchful Waiting Approach simply allows the child to guide their own course and does not immediately confirm that the child’s feelings are their long-term identity.
The Developmental Approach (sometimes called the “therapeutic approach” or “gender exploratory approach”) has the most scientific evidence and allows the child to explore their gender while being open to the possibility that they may grow comfortable in their biological sex. Under the Developmental Approach, a clinician seeks to understand the whole child, including trauma or psychopathology, and what else is going on in the child’s life that makes them feel this way.
The Watchful Waiting Approach and the Development Approach do not attempt to steer a child toward a particular gender identity. In contrast, the Affirmative Approach confirms to the child that their self-diagnosis is correct and pursues significant changes in the child’s life to reflect this. FCPS policy 443, whether by conscious design or a design flaw, steers students to the Affirmative Approach. FCPS may not notify the parent unless the school believes the parents will support it.
We believe this should be a major concern for all parents.
Adolescents with gender dysphoria are more likely than the general population to experience mental health issues, with 40-45% presenting clinically significant psychopathology, compared to roughly 20% of the general population. Abigail Shrier documented multiple stories of biological females who regretted their medical transitions to a different gender identity. They later attributed their decision to transition to other mental health issues that they thought would resolve from the transition but didn’t. A study from the American Journal of Psychiatry showed that 61% of patients presenting with gender dysphoria have another psychiatric disorder, and in 75% of these patients with a psychiatric disorder, gender dysphoria was a symptom of another mental illness.
The bottom line is that by supporting an affirmative-only approach, by design or inadvertently, FCPS may not be taking the time to truly understand children as individuals and this has the potential that this therapy may not be the best for the child. A female adolescent who never had gender-related concerns in childhood and rapidly developed gender dysphoria after experiencing a traumatic event or after several of her friends identified as transgender needs different therapy than a male kindergartener who presented a classic case of child onset gender dysphoria. We don’t believe that “one size fits all” and believe parents who know their child far better than schools should be informed about their child’s gender dysphoria and be able to choose the therapy that best fits their child’s unique needs.
For parents who feel they need to seek professional assistance, we recommend they consider reading Gender Dysphoria: A Therapeutic Model for Working with Children, Adolescents and Young Adults which was written by two clinicians who worked at the UK’s gender clinic.
Part 1: Under policies and state guidelines now in place schools can exclude parents from any conversations about their child’s decisions regarding gender and/or social and medical gender transitions. We believe this is wrong The more parents know the better they can be prepared to support changes that require they be included. We are providing an eight week educational series designed to make sure parents know the facts.
Gender Dysphoria is a condition that describes a person experiencing a sustained and marked difference between their inner sense of being male or female and their biological sex. The Diagnostic and Statistical Manual (called the DSM-5) is the primary psychological reference used by mental health professionals and requires that people be evaluated for at least six months before a mental health condition can be confirmed. For Gender Dysphoria this clinical diagnosis includes multiple conditions that must be evident continuously during this extended period. It can afflict people of any age, but for children, it is typically found in males between the ages of 3-7 and historically has been rare, occurring in 1 out of every 10,000 males. Only in the last ten years have adolescent females been experiencing gender confusion or dysphoria in large numbers.
If a child wants to change their pronouns or consistently exhibit behaviors not traditionally aligned with their biological sex, they may or may not be experiencing gender dysphoria. When gender dysphoria is suspected, psychologists usually take a family history by interviewing both the parents and the child, and a clinical diagnosis is developed that best supports the child and the family’s situation.
Unfortunately, both FCPS and Montgomery County public school (MCPS) policies take the position that they will not notify a parent that their child expressed gender-related concerns at school. What’s more, FCPS and MCPS policy states that they will support a controversial psychosocial intervention for these children and can do so without seeking parents’ permission (see our new article, Gender Choices and the Battle of Biology here). Why would FCPS do this? We’ll explain, in detail, why this is the case later in subsequent versions of this weekly series.
#14: Is Gender Dysphoria the Same As Being Transgender?
No, experiencing gender dysphoria and having an established transgender identity are two different things. Historically the most common presentation of gender dysphoria has been in boys, usually ranging from 3-7 years old, who felt as though they were really females (however the trend is shifting towards females; more on that later in the series). This is called “child onset gender dysphoria” by the DSM-5, the main psychological reference used by mental health professionals. In reviewing ten studies of gender dysphoric children, ~80% of children no longer experienced gender dysphoria at or after puberty and will ultimately identify as their biological sex. The remaining ~20% continue to experience gender dysphoria and/or identify as transgender (the opposite sex) or another gender identity (such as “non-binary”).
When a person’s gender identity returns to match their biological sex, this is called “desistance” in the medical literature. Different studies have found different desistance rates ranging from 61%-98%. A universal rate of desistance has not been determined. The evidence to date strongly suggests that most children experiencing gender dysphoria will identify as their biological sex if they go through puberty and that even children with severe dysphoria can desist. (See Soh, Debra, The End of Gender, Prentice Hall, 2020, page 145). Among those whose gender dysphoria recedes at or through puberty, studies have found more than half will identify as homosexual or bisexual. In other words, the most likely post-puberty outcome for a gender dysphoric child is to identify with their biological sex and be homosexual, not transgender.
Some people do go on to have an established, lifelong transgender identity, and we at Transparency in Education want to be clear that we are not suggesting that ultimately identifying as transgender is an invalid outcome. But we are saying that the available scientific evidence supports the idea that a child who is experiencing child onset gender dysphoria and believes they have a transgender identity is likely not to have that identity if they are allowed to go through puberty. Parents may be interested in watching this 60 Minutes Australia report about a 14-year-old biological male who once identified as female but now identifies as male.
If you have any questions or concerns, please contact us here: [email protected].